

Abstract
Background: Acute myeloid leukemia with myelodysplasia-related changes (AML-MRC) includes a history of myelodysplasia syndrome (MDS) and no MDS history (30% of AML, MDS-related cytogenetic abnormalities, and multilineage dysplasia) which was called MDS-like AML. We assume that traditional AML therapy combined with decitabine (DAC) may improve the effectiveness. We retrospectively analyzed 98 patients diagnosed as MDS-like AML and evaluated the curative effect and side effects of decitabine combined chemotherapy comparing to standard 3+7 induction protocol.
Patients and methods:This study analyzed AML patients aged 14-60 (exclude M3) diagnosed between 2014 to 2017. All patients were supposed to be on at least one of the conditions below: ① anemia, leucopenia, or thrombocytopenia for over 6 months; ② macrocytic anemia (MCV>95.0fL); ③ observation of marrow dyshaematopoiesis; ④immature cells >20% but with low percentage; ⑤FISH detected 5q-, 7q-, +8 or 20q-; ⑥methylation related gene mutation. Ninety-eight eligible patients were included (51 in DAC group; 47 in non-DAC group). 1. DAC group: 22 patients were treated with DAC+CAG, which included decitabine of 20 mg/m2 intravenously d1-5 and G-CSF of 300μg/day (d0-9) for priming combined with cytarabine of 20 mg/m2 for d3-9, aclarubicin of 7 mg/m2 d3-6. 29 patients received DAC+IA/MA regimen (IA for 25 cases, MA for 4 cases), included decitabine of 20 mg/m2 intravenously d1-5 combined with a standard "3+7" induction chemotherapy using standard dose of cytarabine (100 mg q12h) intravenously for day1-7 with idarubicin or mitoxantrone of 8 mg/m2 d1-3. Non-DAC group: all 47 patients were treated with standard 3+7 induction chemotherapy using cytarabine combined with idarubicin or mitoxantrone (IA for 41 cases, MA for 6 cases, the dose and usage are the same as before).
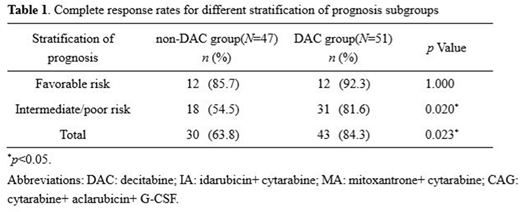
Results:In DAC group, the overall response rate after first course of induction therapy was 90.2%vs. 78.7% in non-DAC group, including 84.3% CR vs. 63.8% in non-DAC group (p=0.023). Curative effects in favorable prognosis group showed no pertinence to decitabine (85.7% vs. 92.3%, p=1.000). The decitabine combined therapy showed a favorable inductive remission rate of 81.6% in intermediate- or high-risk patients, while 54.5% in non-DAC group (p=0.020) (Table 1). Six patients were DNMT3A mutation positive in DAC group,. After the first course of chemotherapy, 4 reached CR (CR%=66.7). 16 patients were TET2 or ASXL1 mutation positive, with respective remission rate of 81.3% and 87.5% at the end of the first course. On hematologic toxicities, comparing with non-DAC group, the combined therapy did not extend the duration of agranulocytosis (p=0.0965) and platelet recovery time (p=0.1335). Relatively, DAC+CAG protocol had reduced the amount of infused suspension of red blood cells. Infection incidence showed no obvious difference between groups.
Conclusions:Decitabine combined chemotherapy could improve the inductive remission rate on MDS-like AML patients under 60 years old in the first course.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal